Vicarious trauma, compassion fatigue and burnout: Tools for EMDR therapists
Vicarious trauma, compassion fatigue and burnout: Tools for EMDR therapists
Lee Anna Simmons & Oliver Wright
Main image: photo by Mark Covell
Share
ctrl / cmd + p or File > Print
This article shares key learning points from the authors’ vicarious trauma training sessions over the last ten years. We include definitions of vicarious trauma, how to identify and guard against it and a catalogue of resources that therapists can use for their own well-being and in their recovery from it.
Our belief is that all EMDR therapists should have a good understanding of vicarious trauma and maintain awareness of it in their daily practice. The self-care recommendations, resources and tools shared in the accompanying article are essential to limit therapists’ exposure to vicarious trauma and to repair any damage taken on in their nervous systems. This approach may improve the lives of therapists and help to prolong therapeutic careers.
Introduction
Vicarious trauma (VT) is a common experience and a predictable risk for EMDR therapists due to the high percentage of clients seeking EMDR for posttraumatic stress disorder (PTSD) or complex PTSD.
The content of this article was presented at our EMDR UK training session, ‘EMDR, VT and Self-Care’ (21 April 2023). The aims are to raise awareness of VT so that therapists can recognise it in the early stages and to share methods practitioners can use to protect themselves and their colleagues and recover from the impact of a high caseload of trauma work. Reference material, insights and resources are shared from the authors’ experiences and research as well as from the contributions of training participants over previous courses and workshops, held by both authors over the last ten years. This includes but is not limited to EMDR therapists, case workers, volunteers, and activists (see acknowledgments).
We have been driven to collate these resources due to the importance of the subject and therefore intend for the information and strategies to be freely shared. Feedback from participants in trainings and workshops has highlighted the importance of collaboration and sharing knowledge with peers, self-care, healthy boundaries and fostering an environment where feelings, experiences and ideas can be safely discussed.
As Babette Rothschild (2006) said, “The first goal of trauma recovery should and must be to improve your quality of life on a daily basis.”
Definitions
There are various words and phrases that are often included under the heading of VT.
In this article the term VT is considered as meaning the trauma that one experiences through empathy and imagination because of things that happen to someone else. VT is sometimes used to describe a shift in one’s sense of self and world view or even one’s spiritual world view. For instance, it was used by Pearlman and Saakvitne (1995) to describe the profound shift in world view that occurs in helping professionals when they work with individuals who have experienced trauma. Helpers notice that their fundamental beliefs about the world are altered and possibly damaged by being repeatedly exposed to traumatic material.
The term secondary trauma is used here for the times that we are traumatised by hearing stories and seeing images. Secondary trauma could occur immediately by being with someone, for example, when a client tells us something shocking and the experience stays with us and affects us after the session. In more extreme cases we could have PTSD symptoms, for example nightmares in the days following the session. Although this article refers to the clinical environment, secondary trauma is not always work related.
The term compassion fatigue refers to the emotional and physical exhaustion that can desensitise us as caring professionals to other people’s needs so that we lose the ability to have empathy for our clients.
Burnout is considered as the point at which a previously committed therapist disengages from their profession in response to the accumulation of stress, compassion fatigue or secondary trauma. Burnout is typically experienced as mental, emotional, and physical exhaustion that results in apathy and indifference toward the helping profession. Therapists can feel helpless or hopeless about their ability to help their clients (Schwartz, 2017).
Recognising vicarious trauma
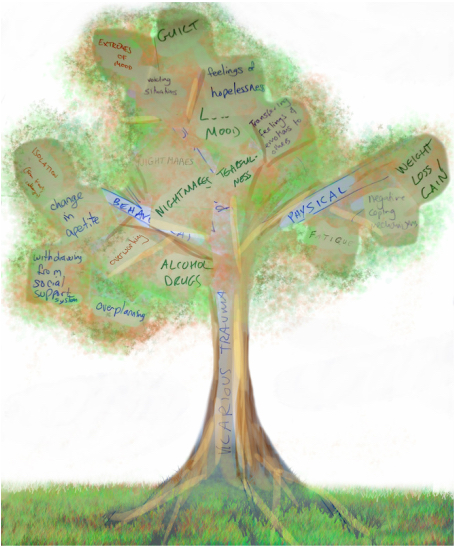
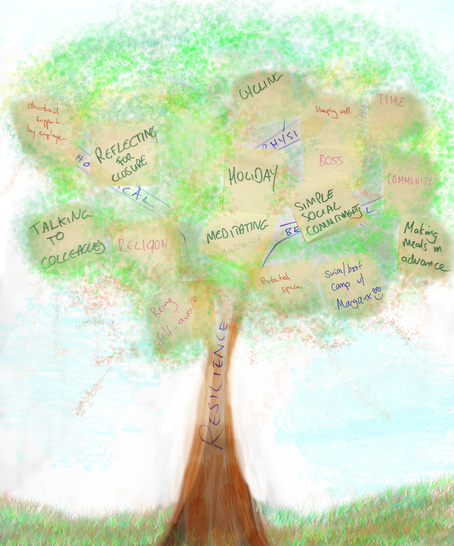
Symptoms of VT can be behavioural, physical or emotional, and all impact the therapist in different ways. Below are two visual representations. Image 1 is of symptoms of VT and image 2 is of methods to guard against it. These trees were created during an early workshop at Doctors of the World UK (DOTW) which works to improve access to healthcare in the UK and internationally. Attendees included volunteers, medical doctors, therapists and office staff. This was a pilot project running training and self-care workshops for volunteers and staff at DOTW and expanded to include their allied organisations.
Image 1. Symptoms of VTImage 2. Guarding against VT
A team at Latin American Womens’ Rights Services (LAWRS) who took part in the project at Doctors of the World, made up of caseworkers, therapists, management and office workers had broadly similar responses. The programme at DOTW started off with information sharing and psychoeducation on VT then developed to themed workshops such as mindfulness, compassion-focused work, coping mechanisms, boundaries, reflective writing and techniques from EMDR and art therapy such as painting the safe place and using bilateral brushstrokes.
Image 3. Bilateral brushstrokes – Angel by L.A.Simmons (2014) oil paint on linen: 170x200cm
In all the VT training sessions that we have been involved with so far, attendees have found it helpful to hear from each other about their experiences and coping strategies.
Guarding against vicarious trauma
Building resilience is a typical way to protect oneself from vicarious and secondary trauma. Trainings at the British Association of Art Therapists (BAAT) and the Headington Institute have emphasised resilience in mitigating the impact of VT. Resilience is defined in the Oxford Dictionary as “the capacity to recover quickly from difficulties; toughness. The ability of a substance or object to spring back into shape; elasticity.” However, we are human, and resilience alone is not sufficient if the therapist’s caseload is overwhelming. After all, if you are in a flood, you are likely to drown. To be sustainable, resilience must be balanced with viable working environments and support structures. Resilience is a substantial and evolving subject which we refer to here for pragmatic signposting only.
Workplace strategies
Having clinical supervision separate from management supervision, where clinicians can voice their concerns about caseload, personal triggers and concerns about safety of practice
Confidential institutional support
Self-care strategies including taking time off, asserting boundaries and training in VT to be able to recognise it in oneself and in colleagues
Inviting colleagues to take relevant training. (There are some great training resources online and for free via the Headington Institute).
Self-care
Babette Rothschild’s excellent book (2006) has some strategies for therapist self-care. For example, she advises therapists not to mirror the client’s body posture too closely as this can make the therapist feel what the client is feeling in a much more intense way – a kind of somatic empathy. For example, when a client slumps in their chair and their breathing becomes shallower, we often find ourselves unconsciously copying them. We may also start to feel hopeless because our body is experiencing what they are feeling. Although many therapists have been trained to mirror with clients, Rothschild suggests that this is no longer helpful if the therapist becomes too dysregulated and cannot then use their own nervous system to help ground the clients.
She advises therapists to be mindful of their body-mirroring, posture, facial-mirroring and breath during sessions and suggests that if the therapist notices themself slumping with their client, they should try:
Lengthening their spine
Cross or uncross their legs
Change their breathing to longer, deeper breaths
Having a drink
Writing some notes
Stretching or change position in their chair
Tensing specific muscles
Exhaling.
Oliver has found this to be one of the most helpful ways of reducing the VT that he experienced from his clients. Lee has also found it helpful to maintain objectivity with highly charged communications both in therapy sessions and with supervisees.
Self tapping bilateral stimulation (BLS) is another good way of staying grounded during an intense session and can be done very subtly out of view when working on Zoom. Some EMDR therapists also choose to accompany their client by using the butterfly hug (shoulder taps) during EMDR sessions and thigh taps with the Flash or Blink technique.
Setting and maintaining boundaries
During the Doctors of The World project, there was some debate about the ethical dilemma of choosing to leave someone homeless or providing them with shelter by opening one’s personal space. Maintaining professional boundaries meant fulfilling their responsibilities by offering more limited support to hundreds of refugees and migrants in their designated roles. For example, an attendee felt an intense urge to blur these boundaries by offering their own home. It was agreed that in this context such an act, although compassionate, would likely prevent the worker from effectively supporting a larger number of people in need.
Managers are often well placed to address VT and promote emotionally sustainable practices. Here are a few examples of management practices that prioritise these aspects.
Organisation
Emotionally sustainable management practice
Benefits
Doctors of the World (DOTW)
Conducts debrief sessions at the end of every clinic day
Allows team members to reflect on their experiences, share information about patients’ needs and the challenges they have faced. This helps to mitigate the impact of VT because workers are better able to leave the work at work, knowing they were not the only person aware of their service user’s predicament.
Community Action for Refugees (CARAS)
Provides independent supervision for team members
Independent supervision offers a dedicated space for clinicians to discuss their work, explore their emotional responses and receive guidance and support from a supervisor. It helps ensure that clinicians have a confidential outlet to address any VT they may experience while providing services.
Freedom from Torture
Joined-up approach with related services
Working with agencies such as legal and social work facilitates collaboration and information sharing. Enhances the support available and ensures access to resources and expertise.
Freedom from Torture
Training in VT Provides independent supervision for staff
Equips clinicians with knowledge and tools to recognise, manage, and mitigate the impact of VT. It also promotes self-care practices and resilience-building techniques to support the emotional well-being of the team.
Freedom from Torture
Caseload management and trigger support
Keeps caseloads within designated limits. Supports clinicians by considering their triggers and helping them avoid working with clients whose situations closely align with those triggers such as traumatic bereavement or fire-related trauma. This practice also demonstrates sensitivity and a commitment to staff emotional well-being.
Table 1. Examples of emotionally sustainable management practices
We have witnessed these examples first hand. They illustrate how managers can prioritise the emotional sustainability of their team members and create a supportive environment that addresses VT. Implementing these practices can contribute to the well-being and effectiveness of the clinicians and ultimately improve the quality of care provided to clients. We believe that even half a day of psychoeducation on VT in core training for therapists, especially for trauma therapists, may have significant benefits and would be straightforward to do. This could involve providing resources and further information in the field, as well as emphasising the importance of strong supervision and self-care practices and by doing so, it is likely to reduce cases of burnout, decrease time off on sick leave, and even prolong careers in the caring and helping professions.
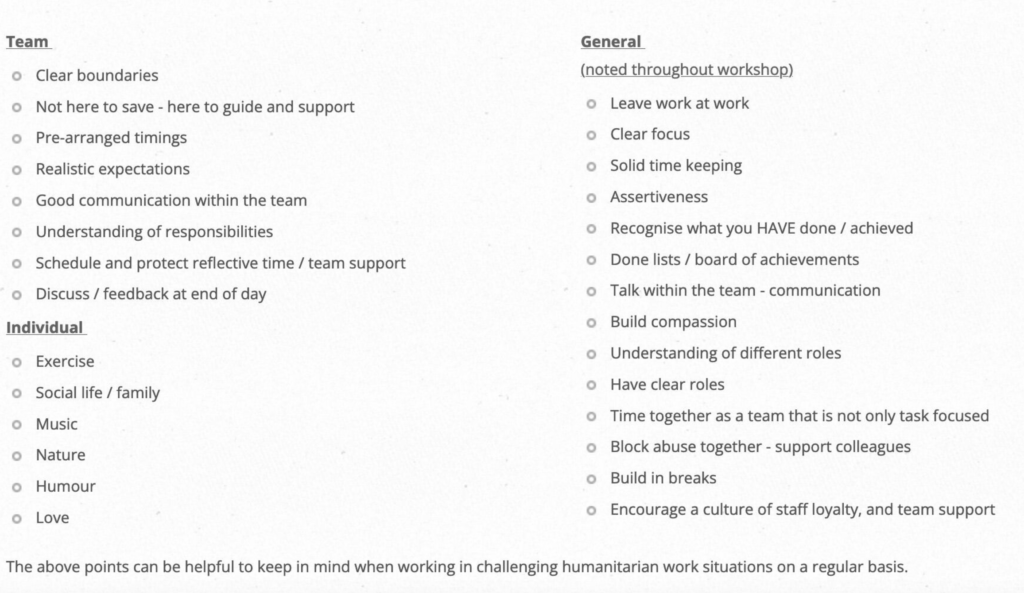
Some key points from humanitarian workers from DOTW and LAWRS are included in the table below:
Table 2. Guarding against VT
Healing vicarious trauma: personal stories
Oliver
During his time at the Grenfell Health and Wellbeing Service since 2017, Oliver has been part of a number of staff wellbeing initiatives. Just like any team working with traumatised clients the team have been impacted by VT. Oliver often noticed feeling exhausted at the end of the working week, sleeping badly, or having nightmares related to the work. Even though generally morale was high, colleagues talked about burnout and compassion fatigue and sometimes secondary trauma. The service had a wellbeing team looking at the impact of the work on staff members and organising social events along with wellbeing activities like yoga, mindfulness and even occasionally massage sessions if a member of staff wanted to offer that to colleagues.
Oliver and his colleagues offered the Group Traumatic Episode Protocol (GTEP) to the entire team. GTEP, developed by Elan Shapiro, is a group EMDR process that allows participants to undergo EMDR simultaneously without disclosing their personal trauma to others in the group or the GTEP therapists. Oliver and other GTEP trained therapists have so far delivered four GTEP sessions for Grenfell staff including both face to face and online sessions. Outcomes from participants have generally seen a drop in SUD of between two and four points in one GTEP session. Staff were also offered various options for continuing with one-to-one EMDR therapy if they wanted to continue working on traumatic material after the session.
Lee
In 2019, Lee was working as an independent consultant for a group of psychodynamic therapists supporting unaccompanied children. She responded to an urgent request to supervise these therapists. The initial supervision sessions were highly emotional. Containing meditations helped ground the therapists as well as teaching them methods that they could use to self-soothe and share with their clients, for example, light stream, container and the four elements grounding exercise from GTEP. The clinicians were supportive of each other and gave kind, honest and helpful feedback. They did not know each other prior to this despite working in the same organisation, but they formed alliances within the supervision group and continued to support each other outside of the meetings.
Lee held a GTEP session with this group to help them manage the traumatic endings they were working with and to prevent the PTSD symptoms that they were reporting from developing further. Tears of desperation and exhaustion were a common feature in early supervision sessions. This did not happen after the group GTEP session. The therapists also worked on asserting boundaries with their clients and with management, protecting the space for clinical work and planning endings in a contained and proactive way.
At the time of writing this article Lee noticed some early signs of VT within herself, having taken on a high level of child cases for EMDR. The steps she took to prevent this from escalating included booking additional one-to-one supervision with a child and adolescent EMDR consultant, making time for this piece of writing and taking a weekend off for her own personal life.
Editing the article a week later, Lee had been working on outdoor activities in South Wales with school children and felt her resilience and resources had bounced back to 80% or even 90%. A strategy she has instigated is to have a proportion of work with children who are generally well and colleagues from a different discipline (in this case outdoor instructors). This allows for a rapid re-set because trauma and suffering are no longer the norm in this group of people. Physical activity, time in nature away from technology and with ‘out of office’ on all contributed to recovery. Ironically, Thai Oil that Muay Thai boxers use in pre and post-fight massages, that Lee has sworn by since her martial arts years in her 20s, was not needed on a full week of sports activities and sleeping in a tent, but she did use it on her shoulders in the week leading up to it when working at the desk and in the clinic full time.
Conclusion
We will not all want or be able to go and work as climbing instructors and sleep in tents, but we can think of ways to balance our workloads with time, people and experiences that can complement and counteract each other. Therapists need to prioritise their own mental health. Just as athletes protect their physical well-being knowing it is crucial for their performance, therapists’ emotional well-being directly impacts their ability to provide effective care.
Rebecca Kase presented on the integration of polyvagal theory with EMDR at the EMDR UK national conference in Glasgow this year. We think that one of the most important things that she had to say was that as therapists we “lend our nervous system to our clients in each session and so we are duty bound to look after it for ourselves and for our clients.”
We also believe that supervisors play a vital role in this regard by being mindful of VT and working with supervisees on establishing boundaries, maintaining a manageable caseload, prioritising personal therapy, and raising awareness of their own triggers. Respecting self-care and safeguarding supervisees’ well-being is essential.
Integrating information on VT into core trainings and providing ongoing support through supervision, can support therapists and mental health workers in developing the necessary awareness and skills to navigate the challenges associated with their work, while prioritising their own mental health.
Having read this far we hope that you have been inspired towards self-care. At the end of our trainings we always ask the participants to consider the following, and we invite you to do the same:
What are some steps that you can take to overcome symptoms of VT?
What are some steps that you can take to guard against symptoms of VT?
Choose one thing to focus on from your answers to these questions to try out for the next week.
Resources to support EMDR therapists’ self-care can be found here.
Acknowledgements
Key partners from past trainings include Phil Murwill clinic/office manager of DOTW and Dr Jennifer Hall, independent consultant/clinical psychologist in the VT trainings held by Doctors of The World and their allied organisations. Naomi Press who supported a workshop for activists held by AntiUniversity, attendees at EMDR and Art Therapy trainings held by the British Association of Art Therapists, Social Art Therapy Ltd and British Association of Dramatherapy, which included a significant section on vicarious trauma. Post-doc students at Imperial and Kings College who contributed to a workshop on self care during the Covid pandemic. Goldsmiths University who commissioned a talk and workshop on vicarious trauma for staff and students together and Second Floor Studios and Arts who commissioned three workshops for artists.
The participants at these vicarious trauma-informed trainings and workshops with Lee, contributed ideas and information that informed her further sessions.
Lee Anna Simmons is an EMDR consultant and art psychotherapist working with adults and children through her company Social Art Therapy Ltd, as well as for the social services, schools, charities and NGO's. She has an active art practice and includes rock climbing in some of her trauma recovery work.
Oliver Wright is an EMDR consultant and works as a senior therapist and supervisor for the NHS Grenfell Health and Wellbeing Service (GHWS) with the community affected by the Grenfell fire. He has nearly 20 years’ experience as a therapist in the NHS and in private practice.
References
Summary of the initiative at DOTW: [PDF]. (n.d.). Retrieved fromhttps://www.socialarttherapy.com/uploads/5/4/4/9/54498927/dotw_vt_self-care_sessions_summaryjh_ls.pdf
Rothschild, B. (2006). Help for the helper: The psychophysiology of compassion fatigue and vicarious trauma. Norton Professional Books.
Schwartz, A. (2017). Preventing therapist burnout. Retrieved fromhttps://drarielleschwartz.com/preventing-therapist-burnout-dr-arielle-schwartz/
Rothschild, B. (2006). Help for the helper: The psychophysiology of compassion fatigue and vicarious trauma. Norton Professional Books.
Share your expertise: contribute to EMDR Therapy Quarterly
We're always looking for new authors. If you've seen, read or developed something in the EMDR field, we'd love to hear from you.
We would love to hear what you think about EMDR Therapy Quarterly and publish your letters on our letters page in each edition. If you have comments or opinions about any of the articles you read here, please let us publish them. Write to: editor@emdrassociation.org.uk
Healthcare professionals are at high risk of vicarious trauma and burnout, especially those who work in inpatient psychiatric settings. This report of a service evaluation demonstrates the benefit of introducing a single session G-TEP to help traumatised staff who might not otherwise present.